-
Centre of Excellence
Specialties
Treatments and Procedures
 HyderabadCARE Hospitals, Banjara Hills CARE Outpatient Centre, Banjara Hills CARE Hospitals, HITEC City CARE Hospitals, Nampally Gurunanak CARE Hospitals, Musheerabad CARE Hospitals Outpatient Centre, HITEC City CARE Hospitals, Malakpet
HyderabadCARE Hospitals, Banjara Hills CARE Outpatient Centre, Banjara Hills CARE Hospitals, HITEC City CARE Hospitals, Nampally Gurunanak CARE Hospitals, Musheerabad CARE Hospitals Outpatient Centre, HITEC City CARE Hospitals, Malakpet Raipur
Raipur
 Bhubaneswar
Bhubaneswar Visakhapatnam
Visakhapatnam
 Nagpur
Nagpur
 Indore
Indore
 Chh. Sambhajinagar
Chh. Sambhajinagar Clinics & Medical Centers
Clinics & Medical Centers
-

-

-

-

-

-
Follow Us

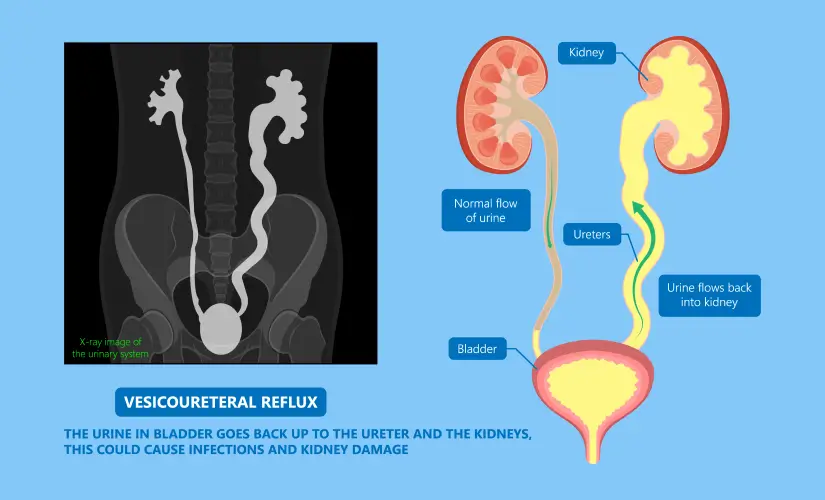
Vesicoureteral Reflux
Symptom, Causes, Diagnosis and Treatment
Vesicoureteral Reflux
Vesicoureteral reflux (VUR) is the most common urological abnormality in neonates. The condition causes urine to flow backwards from the bladder to the kidneys, which substantially raises the risk of kidney damage during UTI.
The condition's root cause often lies in a child's ureter structure at birth. VUR also runs in families, as 30% of an affected child's siblings share the condition. UTIs connected to vesicoureteral reflux can cause lasting kidney damage if left untreated, which makes quick diagnosis and proper management crucial. This article will explain everything you need to understand vesicoureteral reflux, its symptoms, and effective vesicoureteral reflux (VUR) treatment options.
What is Vesicoureteral Reflux?
Vesicoureteral reflux (VUR) happens when urine flows backwards from the bladder up into the ureters and sometimes reaches the kidneys. Urine normally moves in one direction from the kidneys through the ureters to the bladder. Children with VUR have a failed one-way system that lets urine back up, especially when their bladder fills or empties.
Types of Vesicoureteral Reflux
The following are two distinct types of vesicoureteral reflux:
- Primary vesicoureteral reflux: This congenital condition results from an abnormally short intramural ureter that creates a defective valve at the ureterovesical junction. Primary VUR is the most common type that typically affects infants and young children.
- Secondary VUR: This develops because of bladder emptying problems or high bladder pressure. Urinary tract blockages, bladder muscle abnormalities, or nerve damage affecting bladder function can cause it.
Symptoms of Vesicoureteral Reflux
VUR usually doesn't cause pain or direct symptoms. It often guides to urinary tract infections (UTIs) that show up as:
- Fever over 38°C in babies and young children
- Tiredness, irritability and poor feeding in infants
- Pain or burning sensation while passing urine in older children
- Frequent urination or urgency
- Cloudy or foul-smelling urine
Causes of Vesicoureteral Reflux
Primary VUR results from incomplete development of the intramural ureteral tunnel, which causes the normal flap valve mechanism at the ureterovesical junction to fail. The bladder urine flows back into the ureters. Secondary VUR occurs due to increased bladder pressure from outlet obstruction or dysfunctional voiding habits.
Risks of Vesicoureteral Reflux
Your risk of developing VUR increases with several factors:
- Race: White children face a higher risk than Black children
- Sex: Girls generally have a higher risk, but at-birth VUR appears more in boys
- Age: Infants and children under 2 show greater risk
- Family history: Children with parents or siblings who have VUR face increased risk
Complications of Vesicoureteral Reflux
VUR can create serious complications without proper management:
- Kidney scarring from recurrent infections
- Hypertension (high blood pressure)
- Protein in urine (proteinuria)
- Kidney function deterioration
- Kidney failure in severe cases
Diagnosis
A doctor usually starts diagnosing vesicoureteral reflux after a child gets urinary tract infections. These key diagnostic tools help doctors understand the condition:
- Kidney and bladder ultrasound: Uses sound waves to get into the kidney and bladder without radiation exposure
- Voiding cystourethrogram (VCUG): An X-ray test that shows if urine flows backwards while the bladder empties
- Nuclear scan: Uses tracers to review how the urinary tract functions with less radiation than VCUG
- Doctors grade VUR from 1 to 5 based on these tests. Grade 5 shows the most severe form with kidney swelling and twisted ureters.
Treatments for Vesicoureteral Reflux
The severity of the condition determines treatment options. Many children with mild primary VUR naturally outgrow it, so doctors often suggest watching and waiting while taking preventive steps.
Serious cases need these treatments:
- Antibiotic therapy: Low-dose antibiotics to prevent UTIs until the child outgrows the condition
- Surgical correction: Needed when reflux doesn't improve or infections continue despite antibiotics
Surgery options include open surgery through an abdominal incision, robot-assisted laparoscopic surgery using small incisions, and endoscopic surgery that uses gel injection around the affected ureter without external incisions.
When to See A Doctor
Your child needs immediate medical attention if these UTI symptoms appear:
- Strong, persistent urge to urinate
- Burning sensation during urination
- Stomach, groin or side pain
- Upset stomach or vomiting
- Babies younger than 3 months need emergency care if their rectal temperature reaches 100.4°F (38°C) or higher.
Prevention
Parents can't prevent vesicoureteral reflux, but they can help maintain their child's urinary tract health through these steps:
- Give adequate fluids based on the doctor's recommendations
- Maintain good bathroom habits with urination every 2-3 hours
- Address constipation quickly since it raises infection risk
- Change diapers right away for non-potty-trained children
- Take all prescribed antibiotics for UTIs, even after feeling better
- Address related conditions like urinary incontinence
- Prenatal Checkup
Conclusion
Vesicoureteral reflux is a vital urological concern that affects many infants and young children worldwide. This condition increases the risk of recurring urinary tract infections that can damage the kidneys over time, even though it's not painful by itself. Early diagnosis makes a huge difference, as many children with mild cases outgrow the condition without surgery. Parents who know the warning signs of UTIs can get medical help quickly before complications arise.
FAQs
1. How do you treat vesicoureteral reflux in toddlers?
The treatment approach for toddlers with vesicoureteral reflux depends on the condition's severity. Doctors usually recommend watching and waiting for mild cases (grades I-II) since many children naturally outgrow VUR. Moderate to severe cases may need:
- Daily low-dose antibiotics that prevent UTIs until the reflux resolves
- Treatment of constipation and bladder dysfunction if present
- Surgery for persistent or severe cases
2. At what age does VUR resolve?
Children with lower-grade vesicoureteral reflux typically outgrow the condition by age 5-6. Grade V reflux almost always needs surgical intervention.
3. Is VUR a birth defect?
Primary vesicoureteral reflux is a congenital condition that babies are born with. This happens due to incomplete development of the valve that stops urine from flowing backward. The condition stems from an abnormally short intramural ureter that creates a defective valve at the ureterovesical junction. Secondary VUR develops after birth because of bladder emptying problems or high bladder pressure.
4. Does vesicoureteral reflux go away?
Vesicoureteral reflux often resolves on its own as children grow. Milder grades have better chances of disappearing naturally. Young patients with unilateral reflux show higher chances of spontaneous resolution. According to studies, boys experience resolution 12-17 months earlier than girls.
5. How to care for a child with vesicoureteral reflux?
Caring for a child with VUR requires these key practices:
- Give plenty of fluids
- Teach good bathroom habits, including regular urination
- Treat constipation quickly
- Change diapers often for non-potty-trained children
- Address related conditions like urinary incontinence
6. Does VUR require surgery?
Not every case of vesicoureteral reflux needs surgery. Doctors recommend surgical intervention when:
- Children get repeated UTIs despite taking preventative antibiotics
- High-grade reflux (IV-V) shows no signs of improvement
- Kidney scarring appears or gets worse
- Children develop breakthrough infections while on antibiotic prophylaxis
Treatment options include ureteral reimplantation, endoscopic injection of bulking agents, and sometimes robot-assisted laparoscopic approaches.
7. Is VUR a rare disease?
VUR affects 1-2% of all children, making it a common urological condition. The numbers rise significantly in certain groups - 30-40% of children with febrile UTIs have VUR. Children whose siblings have VUR show higher occurrence rates.
8. What are the five grades of vesicoureteral reflux?
The international system classifies VUR severity from I to V:
- Grade I: Reflux into non-dilated ureter only
- Grade II: Reflux reaches the kidney without dilation of the collecting system
- Grade III: Mild to moderate dilation with minimal blunting of fornices
- Grade IV: Moderate ureteral tortuosity with dilation of pelvis and calyces
- Grade V: Severe dilation of ureter, pelvis and calyces with loss of normal kidney structure
To Book an Appointment, call:
Still Have a Question?
